
Emergency preparedness and a well-rehearsed, coordinated response have never been more important to the health, safety and security of our healthcare organizations, communities or nation. If nothing else, the pandemic proved that healthcare organizations have more work to do on emergency planning.
The American College of Emergency Physicians (ACEP) found that 93% of physicians surveyed do not believe their emergency departments are fully prepared for the influx of patients that follows a disaster or mass casualty incident. Even basic care is compromised, with 90% of physician respondents indicating they do not have access to critical medicine, and nearly 40% stating that patients have been negatively affected as a result. Generally absent from the literature is sterile processing department (SPD) preparedness, not just during a crisis but in day-to-day operations. An SPD emergency could mean several hundred trays down at the start of a new day, a need to reprocess the same several instrument sets to support heavy caseloads, equipment failures, supply shortages, water leaks, temperature or humidity breaches—and the list goes on. When a catastrophic event occurs on top of those other common challenges, it can be a recipe for disaster.

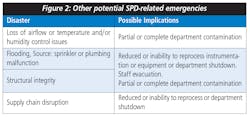
Both natural or manmade disasters of varying degrees can occur daily in the U.S. and can include mass shootings, bombings and terrorism attacks; biohazard-related incidents; civil disturbances; chemical, industrial and hazardous materials emergencies; cybersecurity breaches; disease outbreaks; fires; mass casualty incidents; smoke exposure; utility disruptions, and natural disasters (see Figure 1). Specific to the SPD, leaders should also prepare for the following emergencies: loss of airflow or temperature and/or humidity control issues; flooding (sprinkler or plumbing malfunction); structural integrity issues, and supply chain disruptions, to name just a few (see Figure 2).
What if disaster strikes your facility?
Every disaster poses its own problems, and each disaster may have multiple implications for the department. One disaster may lead to another, for example, amplifying the impact on the department. To mitigate these challenges, SP leaders should incorporate disaster planning into their staff training and orientation processes and manage the disasters promptly and proactively.
It is imperative that SP leaders play an active role in emergency preparedness and that they work to answer the following essential questions:
- Is the organization a standalone hospital, or part of an integrated system where policies and procedures need to be standardized?
- Will the organization increase, curtail or eliminate surgery and other procedures pending disaster support needs?
- Will the facility receive interim help from a sister facility, other healthcare organization or vendor(s)? If such support is available, SP leaders should then consider the support’s proximity to the organization and the timing of that support; whether the support will include the provision of mobile operations or perhaps even transportation, housing and meals (if needed); and any financial implications.
- Who is the emergency coordinator for the department, service line or organization (and who is their backup should they be unavailable)? If the department lacks an emergency coordinator, who should be contacted first if disaster strikes?
- What process should be followed in an emergency—and do all employees know the process? How is prioritization of manpower, equipment and supplies determined and are there checklists employees can follow to ensure proper response to the emergency?
- Which emergency events must be reported (i.e., equipment malfunctions/failures, impact the disaster event may have on other units)?
- Is there an emergency response number employees can call if they become overwhelmed or require other forms of support?
- Are any SP employees serving in the National Guard? If so, how will the department manage if those employees must leave the facility to respond to an emergency outside the facility?
Conclusion
Many healthcare organizations are not well prepared for disasters, and this lack of preparedness threatens communities and our nation’s response capabilities. Emergency events can create confusion and chaos; however, effective management of these incidents is possible when senior and departmental leadership proactively plan for emergencies, targeted employee training and timely, detail-focused disaster response.
About the Author

David Taylor
Principal, Resolute Advisory Group LLC
David L. Taylor, MSN, RN, CNOR is an independent hospital and ambulatory surgery center consultant and the principal of Resolute Advisory Group LLC, in San Antonio, Texas.